Actor Ro Brooks Encourages you to Help us find a cure for Sarcoidosis.
All Donations are appreciated. 100% of the proceeds will be donated to the SARCOIDOSIS RESEARCH FOUNDATION.
Bernard Jeffrey McCullough, better known to his adoring fans as Bernie Mac, was an American stand-up comedian, actor and voice actor. In the final three years of his life, Mac publicly disclosed that he had suffered from sarcoidosis, a disease of unknown origin that causes inflammation in tissue. Sarcoidosis frequently attacked Mac’s lungs. Mac died August 9, 2008 from complications of pneumonia.
Sarcoidosis is a systemic inflammatory disease that can affect any organ, although it can be asymptomatic and is discovered by accident in about 5% of cases.[17] Common symptoms, which tend to be vague, include fatigue (unrelieved by sleep; occurs in 66% of cases), lack of energy, weight loss, joint aches and pains (which occur in about 70% of cases),[18] arthritis (14–38% of persons), dry eyes, swelling of the knees, blurry vision, shortness of breath, a dry, hacking cough, or skin lesions.[19][20][21][22] Less commonly, people may cough up blood.[19] The cutaneous symptoms vary, and range from rashes and noduli (small bumps) to erythema nodosum, granuloma annulare, or lupus pernio. Sarcoidosis and cancer may mimic one another, making the distinction difficult.[23]
The combination of erythema nodosum, bilateral hilar lymphadenopathy, and joint pain is called Löfgren syndrome, which has a relatively good prognosis.[19] This form of the disease occurs significantly more often in Scandinavian patients than in those of non-Scandinavian origin.[24]
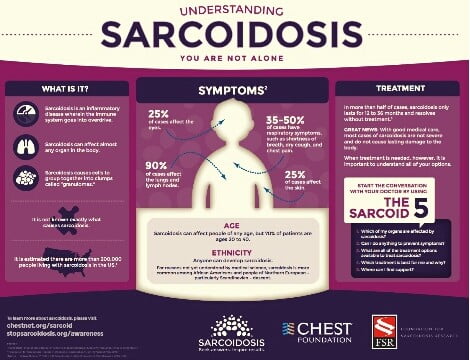
Respiratory Tract
Localization to the lungs is by far the most common manifestation of sarcoidosis.[25] At least 90% of affected persons experience lung involvement.[26] Overall, about 50% develop permanent pulmonary abnormalities, and 5 to 15% have progressive fibrosis of the lung parenchyma. Sarcoidosis of the lung is primarily an interstitial lung disease in which the inflammatory process involves the alveoli, small bronchi and small blood vessels.[27] In acute and subacute cases, physical examination usually reveals dry crackles.[26] At least 5% of persons will suffer pulmonary arterial hypertension.[26][28] The upper respiratory tract (including the larynx, pharynx, and sinuses) may be affected, which occurs in between 5 and 10% of cases.[29]
There are four stages of pulmonary involvement based on radiological stage of the disease, which is helpful in prognosis:[30]
- Stage I: bilateral hilar lymphadenopathy (BHL) alone
- Stage II: BHL with pulmonary infiltrates
- Stage III: pulmonary infiltrates without BHL
- Stage IV: fibrosis.
Use of the Scadding scale only provides general information regarding the prognosis of the pulmonary disease over time. Caution is recommended as it only shows a general relation with physiological markers of the disease and the variation is such that it has limited applicability in individual assessments, including treatment decisions.[31]
Skin
Sarcoidosis involves the skin in between 9 and 37% of persons and is more common in African Americans than in European Americans.[26] The skin is the second most commonly affected organ after the lungs.[32] The most common lesions are erythema nodosum, plaques, maculopapular eruptions, subcutaneous nodules, and lupus pernio.[32] Treatment is not required, since the lesions usually resolve spontaneously in two to four weeks. Although it may be disfiguring, cutaneous sarcoidosis rarely causes major problems.[26][33][34] Sarcoidosis of the scalp presents with diffuse or patchy hair loss.[35][36]
Heart
The frequency of cardiac involvement varies and is significantly influenced by race; in Japan more than 25% of persons with sarcoidosis have symptomatic cardiac involvement, whereas in the US and Europe only about 5% of cases present with cardiac involvement.[26] Autopsy studies in the US have revealed a frequency of cardiac involvement of about 20–30%, whereas autopsy studies in Japan have shown a frequency of 60%.[21] The presentation of cardiac sarcoidosis can range from asymptomatic conduction abnormalities to fatal ventricular arrhythmia.[37][38] Conduction abnormalities are the most common cardiac manifestations of sarcoidosis in humans and can include complete heart block.[39] Second to conduction abnormalities, in frequency, are ventricular arrhythmias, which occurs in about 23% of persons with cardiac involvement.[39] Sudden cardiac death, either due to ventricular arrhythmias or complete heart block is a rare complication of cardiac sarcoidosis.[40][41] Cardiac sarcoidosis can cause fibrosis, granuloma formation, or the accumulation of fluid in the interstitium of the heart, or a combination of the former two.[42][43]
Eye
Eye involvement occurs in about 10–90% of cases.[21] Manifestations in the eye include uveitis, uveoparotitis, and retinal inflammation, which may result in loss of visual acuity or blindness.[44] The most common ophthalmologic manifestation of sarcoidosis is uveitis.[21][45][46] The combination of anterior uveitis, parotitis, VII cranial nerve paralysis and fever is called uveoparotid fever or Heerfordt syndrome (D86.8). Development of scleral nodule associated with sarcoidosis has been observed.[47]
Nervous System
Any of the components of the nervous system can be involved.[48] Sarcoidosis affecting the nervous system is known as neurosarcoidosis.[48] Cranial nerves are most commonly affected, accounting for about 5–30% of neurosarcoidosis cases, and peripheral facial nerve palsy, often bilateral, is the most common neurological manifestation of sarcoidosis.[48][49][50] It occurs suddenly and is usually transient. The central nervous system involvement is present in 10–25% of sarcoidosis cases.[29] Other common manifestations of neurosarcoidosis include optic nerve dysfunction, papilledema, palate dysfunction, neuroendocrine changes, hearing abnormalities, hypothalamic and pituitary abnormalities, chronic meningitis, and peripheral neuropathy.[26] Myelopathy, that is spinal cord involvement, occurs in about 16–43% of neurosarcoidosis cases and is often associated with the poorest prognosis of the neurosarcoidosis subtypes.[48] Whereas facial nerve palsies and acute meningitis due to sarcoidosis tends to have the most favourable prognosis.[48] Another common finding in sarcoidosis with neurological involvement is autonomic or sensory small fiber neuropathy.[51][52] Neuroendocrine sarcoidosis accounts for about 5–10% of neurosarcoidosis cases and can lead to diabetes insipidus, changes in menstrual cycle and hypothalamic dysfunction.[48][50] The latter can lead to changes in body temperature, mood and prolactin (see the endocrine and exocrine section for details).[48]
Endocrine and Exocrine
Prolactin is frequently increased in sarcoidosis, between 3% and 32% of cases have hyperprolactinemia[53] this frequently leads to amenorrhea, galactorrhea, or nonpuerperal mastitis in women. It also frequently causes an increase in 1,25-dihydroxy vitamin D, the active metabolite of vitamin D, which is usually hydroxylated within the kidney, but in sarcoidosis patients hydroxylation of vitamin D can occur outside the kidneys, namely inside the immune cells found in the granulomas the condition produces. 1,25-dihydroxy vitamin D is the main cause for hypercalcemia in sarcoidosis and overproduced by sarcoid granulomata. Gamma-interferon produced by activated lymphocytes and macrophages plays a major role in the synthesis of 1 alpha, 25(OH)2D3.[54] Hypercalciuria (excessive secretion of calcium in one’s urine) and hypercalcemia (an excessively high amount of calcium in the blood) are seen in <10% of individuals and likely results from the increased 1,25-dihydroxy vitamin D production.[55]
Thyroid dysfunction is seen in 4.2–4.6% of cases.[56][57]
Parotid enlargement occurs in about 5–10% of persons.[18] Bilateral involvement is the rule. The gland is usually not tender, but firm and smooth. Dry mouth can occur; other exocrine glands are affected only rarely.[26] The eyes, their glands, or the parotid glands are affected in 20–50% of cases.[58]
Gastrointestinal and Genitourinary
Symptomatic GI involvement occurs in less than 1% of persons (note that this is if one excludes the liver), and most commonly the stomach is affected, although the small or large intestine may also be affected in a small portion of cases.[18][59] Studies at autopsy have revealed GI involvement in less than 10% of people.[50] These cases would likely mimic Crohn’s disease, which is a more commonly intestine-affecting granulomatous disease.[18] About 1–3% of people have evidence of pancreatic involvement at autopsy.[50] Symptomatic kidney involvement occurs in just 0.7% of cases, although evidence of kidney involvement at autopsy has been reported in up to 22% of people and occurs exclusively in cases of chronic disease.[18][21][50] Symptomatic kidney involvement is usually nephrocalcinosis, although granulomatous interstitial nephritis that presents with reduced creatinine clearance and little proteinuria is a close second.[18][50] Less commonly, the epididymis, testicles, prostate, ovaries, fallopian tubes, uterus, or the vulva may be affected, the latter may cause vulva itchiness.[21][60][61] Testicular involvement has been reported in about 5% of people at autopsy.[50][61] In males, sarcoidosis may lead to infertility.[62]
Around 70% of people have granulomas in their livers, although only in about 20–30% of cases liver function test anomalies reflecting this fact are seen.[19][26] About 5–15% of persons exhibit hepatomegaly, that is an enlarged liver.[21] Only 5–30% of cases of liver involvement are symptomatic.[63] Usually, these changes reflect a cholestatic pattern and include raised levels of alkaline phosphatase (which is the most common liver function test anomaly seen in persons with sarcoidosis), while bilirubin and aminotransferases are only mildly elevated. Jaundice is rare.[18][26]
Blood
Abnormal blood tests are frequent, accounting for over 50% of cases, but is not diagnostic.[26][29] Lymphopenia is the most common blood anomaly in sarcoidosis.[26] Anemia occurs in about 20% of people with sarcoidosis.[26] Leukopenia is less common and occurs in even fewer persons but is rarely severe.[26] Thrombocytopenia and hemolytic anemia are fairly rare.[18] In the absence of splenomegaly, leukopenia may reflect bone marrow involvement, but the most common mechanism is a redistribution of blood T cells to sites of disease.[64] Other nonspecific findings include monocytosis, occurring in the majority of sarcoidosis cases,[65] increased hepatic enzymes or alkaline phosphatase. People with sarcoidosis often have immunologic anomalies like allergies to test antigens such as Candida or purified protein derivative (PPD).[58] Polyclonal hypergammaglobulinemia is also a fairly common immunologic anomaly seen in sarcoidosis.[58]
Lymphadenopathy (swollen glands) is common in sarcoidosis and occurs in 15% of cases.[22] Intrathoracic nodes are enlarged in 75 to 90% of all people; usually this involves the hilar nodes, but the paratracheal nodes are commonly involved. Peripheral lymphadenopathy is very common, particularly involving the cervical (the most common head and neck manifestation of the disease), axillary, epitrochlear, and inguinal nodes.[66] Approximately 75% of cases show microscopic involvement of the spleen, although only in about 5–10% of cases does splenomegaly appear.[18][58]
Bone, Joints, and Muscles
Sarcoidosis can be involved with the joints, bones and muscles. This causes a wide variety of musculoskeletal complaints that act through different mechanisms.[67] About 5–15% of cases affect the bones, joints, or muscles.[29]
Arthritic syndromes can be categorized in two ways: as acute or chronic.[67] Sarcoidosis patients suffering acute arthritis often also have bilateral Hilar lymphadenopathy and Erythema nodosum. These three associated syndromes often occur together in Löfgren syndrome.[67] The arthritis symptoms of Löfgren syndrome occur most frequently in the ankles, followed by the knees, wrists, elbows, and metacarpophalangeal joints.[67] Usually true arthritis is not present, but instead, periarthritis appears as a swelling in the soft tissue around the joints that can be seen by ultrasonographic methods.[67] These joint symptoms tend to precede or occur at the same time as erythema nodosum develops.[67] Even when erythema nodosum is absent, it is believed that the combination of hilar lymphadenopathy and ankle periarthritis can be considered as a variant of Löfgren syndrome.[67] Enthesitis also occurs in about one-third of patients with acute sarcoid arthritis, mainly affecting the Achilles tendon and heels.[67] Soft tissue swelling of the ankles can be prominent, and biopsy of this soft tissue reveals no granulomas but does show panniculitis that is similar to erythema nodosum.[67]
Chronic sarcoid arthritis usually occurs in the setting of more diffuse organ involvement.[67] The ankles, knees, wrists, elbows, and hands may all be affected in the chronic form and often this presents itself in a polyarticular pattern.[67] Dactylitis similar to that seen in Psoriatic arthritis, that is associated with pain, swelling, overlying skin erythema, and underlying bony changes may also occur.[67] Development of Jaccoud arthropathy (a nonerosive deformity) is very rarely seen.[67]
Bone involvement in sarcoidosis has been reported in 1–13% of cases.[50] The most frequent sites of involvement are the hands and feet, whereas the spine is less commonly affected.[67] Half of the patients with bony lesions experience pain and stiffness, whereas the other half remain asymptomatic.[67] Periostitis is rarely seen in Sarcoidosis and has been found to present itself at the femoral bone